Article Text

Abstract
Background The enactment of child restraint systems (CRSs) legislation is highly effective in increasing CRS practices. However, evidence from low- and middle-income countries is still lacking. This study aimed to assess the changes in CRS practices in Shenzhen, China following the implementation of CRS legislation.
Methods Data from two cross-sectional surveys conducted in community health service centres and kindergartens 1 year before and 3 years after the enactment of mandatory CRS legislation in 2015 were used to assess the changes in CRS practices in Shenzhen, China. Temporal changes in CRS practices were investigated, and logistic regression models were performed to examine the differences in CRS practices 3 years after the legislation compared with the period before the legislation.
Results The proportion of CRS possession and use increased from 27.8% (1047/3768, 95% CI: 26.4% to 29.3%) to 72.6% (4900/6748, 95% CI: 71.5% to 73.7%) and from 22.9% (864/3768, 95% CI: 21.6% to 24.3%) to 56.3% (3800/6748, 95% CI: 55.1% to 57.5%), respectively, with a decrease of appropriate CRS use from 75.9% (656/864, 95% CI: 72.9% to 78.7%) to 69.7% (2649/3800, 95% CI: 68.2% to 71.2%) after the implementation of CRS legislation.
Conclusions The findings indicate a significant improvement in CRS possession and use in Shenzhen, 3 years after the enactment of mandatory CRS legislation. Further efforts to update the local legislation to provide specific guidelines for appropriate CRS use and implement targeted multifaceted interventions are needed to increase optimal CRS practices for better child passenger safety in Shenzhen.
- Child
- Legislation
- Restraints
Data availability statement
Data are available upon reasonable request. Data of the research are available upon reasonable request from the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Road traffic crashes with high morbidity and mortality remain a serious global public health problem. This is a case in China, where the mortality rate due to road traffic injuries among children less than 14 years old is significantly higher than that in high-income countries. A growing body of literature from high-income countries has indicated that the enactment of child restraint systems (CRSs) legislation is a highly effective way to increase the use of CRS to protect child passengers. However, evidence from low- and middle-income countries is still lacking.
WHAT THIS STUDY ADDS
This is the first study to examine changes in CRS practices among parents in China following the enactment of a local CRS mandatory legislation. Data from two cross-sectional surveys conducted in community health service centres and kindergartens before and after the implementation of the local CRS legislation in Shenzhen were analysed to assess the changes in CRS practices. The results reveal significant increases in parents owning and using CRS, but the appropriate CRS use decreases after the enactment of legislation in Shenzhen, which would be expected to provide data for designing and implementing effective comprehensive countermeasures.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study indicates the positive effect of the local legislation, but there remains ambiguous on the age-appropriate CRS that parents should choose for their children. Further efforts to update the local mandatory legislation and implement targeted multifaceted interventions including increased and sustained enforcement of laws are highly needed to increase optimal CRS practices to realise its full benefit for better child passenger safety. A field inspection study is also needed to evaluate the actual CRS practices. Meanwhile, this study also provides supportive evidence for the introduction of national laws mandating CRS use in China.
Introduction
Road traffic crashes with high morbidity and mortality remain a serious global public health problem. Globally, they are responsible for more than 1.35 million deaths and cause up to 50 million injuries every year,1 2 and are the leading killer of children and young adults aged 5–29 years globally.3 In China, road traffic injuries are the second-leading cause of death for children from 1 to 14 years old,4 and the majority of these are pedestrians and passengers.5 The mortality rate due to road traffic injuries among children less than 14 years old in China is significantly higher than that in high-income countries.6
Extensive studies have shown that child restraint systems (CRSs) are highly effective in reducing the risk of injury and death to child vehicle passengers.7–10 Using CRS while travelling in a motor vehicle, regardless of the type of CRS, contributes to a reduction in road traffic deaths, particularly for children under 4 years old.10 11 As noted in previous studies, using appropriate and correctly fitted CRS is associated with a 71% reduction in the odds of death for infants under 1 year old, and a 54%–80% decrease for toddlers aged 1–4 years in motor vehicle crashes.12 13 Use rates of CRS in high-income countries, ranging from 84% to 95%,14–16 are much higher than those in low- and middle-income countries.17–19
Legislation of mandatory CRS use in line with WHO best practice is a highly effective way to promote the use of CRS.20 However, according to the WHO, only 84 out of 194 countries have a national child restraint law requiring the use of CRS for children in automobiles in 2016.3 In China, there has been limited activity. To date, a national Law on the Protection of Minors which includes text about using CRS without stipulated penalties and some provincial-city-level regulations have been put in place in China to reduce injuries and deaths among child passengers in the event of a road traffic crash, but the use of CRS is between 0.6% and 64.8%.17 21–23
In 2015, the Shenzhen Municipal Fifth People’s Congress amended the road traffic safety regulations of the Shenzhen Special Economic Zone prohibiting children younger than 4 years old from riding in non-commercial passenger vehicles without using a CRS that meets the national standards, and stipulating a 300 CNY (approx. US$41) fine for those not adhering to this law.24 We hypothesise that CRS practices will have changed in Shenzhen following these amendments to road traffic safety laws. The objective of this study, using locally representative data from two population-based cross-sectional surveys conducted 1 year before and 3 years after the enactment of the law, is to assess whether parents have changed their CRS practices over this period.
Methods
Study sample
Surveys were conducted before and after the implementation of the local CRS legislation in Shenzhen to assess the changes in CRS practices. The inclusion criteria for the studies were as follows: families (1) have at least one child from 0 to 6 years old, (2) have at least one private car and (3) consent to participate in the study.
Pre-legislation data were obtained from a cross-sectional study in Shenzhen conducted between April and May 2014. The details of the population-representative study are described elsewhere.25 In brief, nine government-designated community health service centres (places for vaccination of children aged 0–3 years) and eight government-designated kindergartens (places for preschool education of children from 4 to 6 years old) were selected across Shenzhen using cluster randomised sampling.
The post-legislation sample was drawn from a cross-sectional study of CRS practices during January and March 2018 and has also been reported in detail in a previous study.26 Briefly, a total of 20 community health service centres and 28 kindergartens were randomly selected using probability-proportional-to-size cluster sampling. The sample sizes of children aged 0–3 years and 4–6 years were obtained according to the ratio of age from community health service centres and kindergartens, respectively.
Data collection
All data collected from the pre-legislation and post-legislation surveys were used and compared, and the data collection methods in two surveys were identical. Families with children aged 0–3 years who met the inclusion criteria were invited to participate in the survey and answer the questionnaire when they were waiting for vaccination in the community health service centres. For families with children from 4 to 6 years old, the questionnaire was distributed by teachers and taken home by children to parent meeting the inclusion criteria to complete. A brief introduction to the study and questionnaire instructions was given to all participants before they started to complete the questionnaires.
To ensure the methods of investigation and the process of data collection were consistent during the study period, the staff were trained uniformly, including child passenger safety theory, investigation techniques and procedures of data collection. Our trained personnel would answer any question that arose from the participants during the session, and the authors would also deal with problems in a timely manner.
Data were collected on the child’s age and sex; sex and education level of parents who answered the questionnaire; the price of the car they owned, and their knowledge of CRS; whether they owned and used CRS; the type of CRS used; and whether the CRS was set up consistent with the manufacturer’s instructions. The use of seat-belts by the driver and the trip frequency and distance that parents transported their children in cars regularly were also documented.
Variable descriptions and definitions
Raw data from the two cross-sectional surveys were checked, re-coded and categorised as follows. The children’s age was truncated to the last birthday and grouped as 0–1, 2–3 or 4–6 years old. Categories used for the ‘education level’, ‘car price’, ‘seat-belt use’, ‘trip frequency’ and ‘trip distance’ were identical in the pre-legislation and post-legislation samples. School education levels of parents were categorised as a college education or higher and lower than college (between high school and undergraduate in China). The car price was classified into two different groups: high (≤170 000 CNY, approx. US$23 423) and low (>170 000 CNY, approx. US$23 423). Driver’s seat-belt use was defined as the seat-belt is always, often or sometimes used by drivers, while seat-belt non-use as the seat-belt is seldom or never used.
Six questions were used to evaluate parents’ knowledge of CRS. They were identical in the two cross-sectional surveys, which possessed sound reliability in the study (Cronbach’s α=0.754). Parents were asked to choose between ‘correct’, ‘wrong’ and ‘uncertain’ for each question. One point was given for each correct answer and zero for the wrong ones. The total scores were calculated based on the participant’s responses and then the participants were grouped into two groups, viz. low (ie, ≤3 points) and high (ie, >3 points). Higher scores indicated a greater level of CRS knowledge.
The types of CRS were coded as rear-facing, forward-facing, booster (which may have a back or be backless and is used with a vehicle’s seat-belt or accessory harness) or other.
Four outcome variables were constructed. ‘CRS possession’ was based on parents’ reported ownership of CRS for child occupants. ‘CRS use’ was defined as the CRS being used always, often or sometimes, and CRS non-use as seldom or never used or did not have CRS. The use of CRS was coded as ‘appropriate’ or ‘inappropriate’ according to the China regulation for Restraining devices for child occupants of power-driven vehicles.27 ‘Correct CRS use’ was defined as CRS reported to be used and installed according to the manufacturer’s instructions. Appropriateness and correctness of CRS usage were assessed only among those who used child restraints (ie, those reporting CRS use always, often and sometimes).
Statistical analysis
Categorical data were expressed as numbers and percentages (95% CIs) and compared by χ2 tests for group differences between the pre-legislation and post-legislation samples. Logistic regression models were applied to examine the changes in CRS practices between pre-legislation and post-legislation. Given the fact that these surveys were cross-sectional but not cohort studies, collected across different samples and different periods, there may be several uncontrolled factors that might influence the results. Thus, sets of sensitivity analyses for ORs for CRS possession and usage were conducted to test the stability of the results. First, considering that differences in CRS practices may occur between various demographics, subgroups analysis was performed. Second, different models with progressively increased adjustments for different numbers of variables were undertaken. A two-sided p value <0.05 was considered statistically significant, and all statistical analyses were conducted using SPSS V.23.0.
Results
The characteristics of participants in each survey are presented in table 1. There were 3768 participants from 17 pre-legislation sites and 6748 from 48 post-legislation sites. The post-legislation sample had older children and a higher proportion of female parents reporting data and owned more expensive cars (all p≤0.001), while the education level of parents who answered the questionnaire was higher in the pre-legislation sample (p<0.001). Moreover, more pre-legislation parents transported their children more frequently, but more of these children were transported on either very short trips (<5 km) or trips of 10 km or more each time by found post-legislation (both p<0.001). In addition, higher knowledge scores for CRS were seen in the post-legislation sample (p<0.001).
Comparisons between the pre-legislation and post-legislation samples in Shenzhen*†
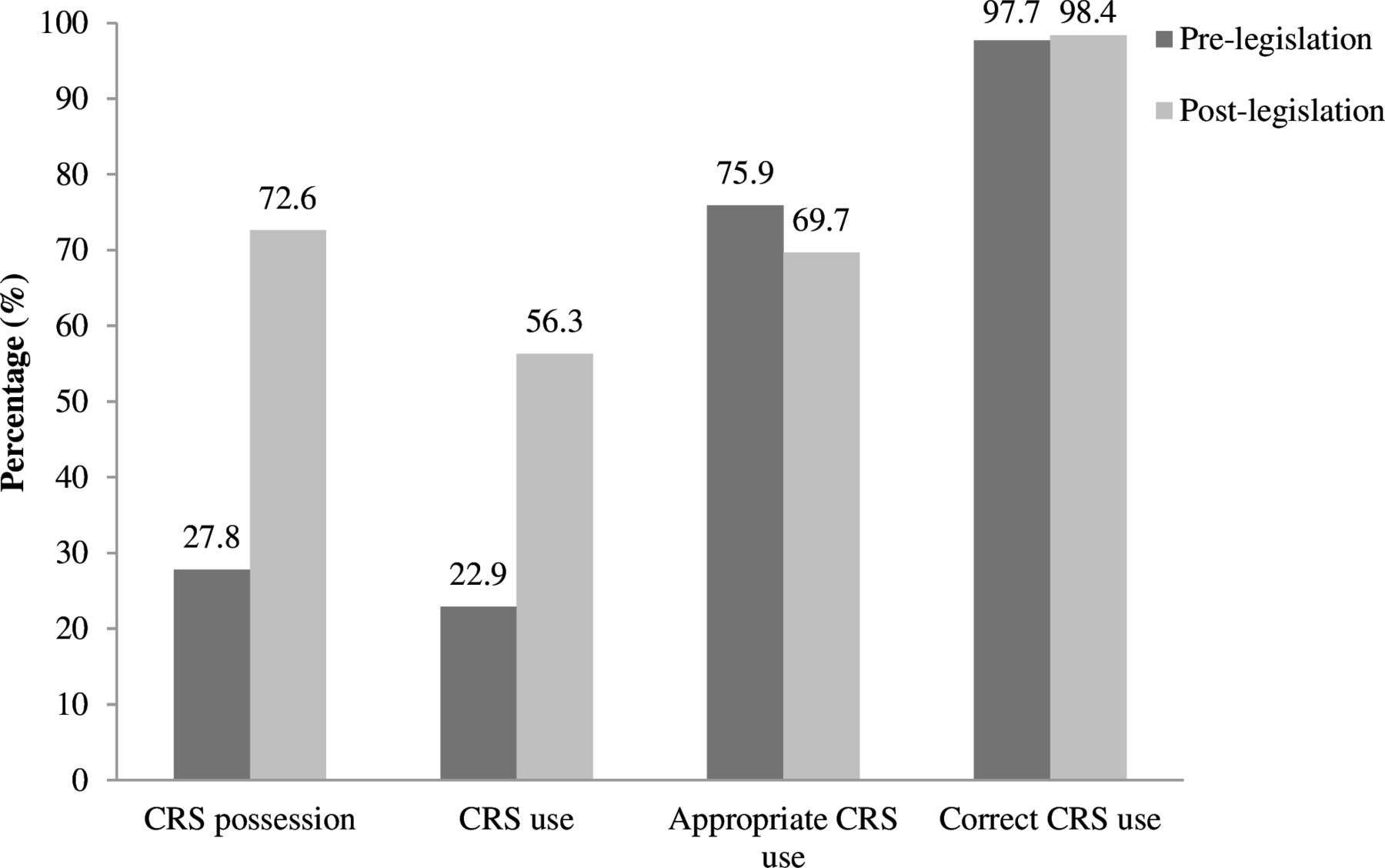
Overall, compared with pre-legislation, the proportion of parents who owned CRS (72.6% (4900/6748, 95% CI: 71.5% to 73.7%) vs 27.8% (1047/3768, 95% CI: 26.4% to 29.3%), p<0.001) and restrained their children with CRS (56.3% (3800/6748, 95% CI: 55.1% to 57.5%) vs 22.9% (864/3768, 95% CI: 21.6% to 24.3%), p<0.001) was significantly higher in the post-legislation sample. Meanwhile, the portion of parents using CRS appropriately decreased from pre-legislation 75.9% (656/864, 95% CI: 72.9% to 78.7%) to post-legislation 69.7% (2649/3800, 95% CI: 68.2% to 71.2%) (p<0.001). There was a higher but non-significant proportion of reported correct CRS use among the overall population after the enactment of legislation (98.4% (3738/3800, 95% CI: 97.9% to 98.7%) vs (97.7% (844/864, 95% CI: 96.4% to 98.6%), p=0.168) (figure 1).

Comparison of CRS practices in the pre-legislation and post-legislation samples in Shenzhen. CRS, child restraint system.
The results of the sensitivity analysis by subgroups on the changes in CRS practices in Shenzhen are displayed in table 2 and show significant differences between subgroups. Remarkable increases in CRS possession and use could be found in children aged at least 2 years compared with their counterparts. There was an increase in appropriate CRS use among children aged below 3 years, but an opposite trend could be observed in other age group. Furthermore, tables 3 and 4 show that the changes in the rates of CRS possession, use and appropriate use remained stable in three logistic regression models after controlling for various numbers of potentially confounding variables.
Changes in CRS practices in the pre-legislaion and post-legislation samples in Shenzhen by subgroups*
Unadjusted ORs (95% CIs) for changes in CRS practices between pre-legislation and post-legislation in Shenzhen
Adjusted ORs (95% CIs) for changes in CRS practices between pre-legislation and post-legislation in Shenzhen
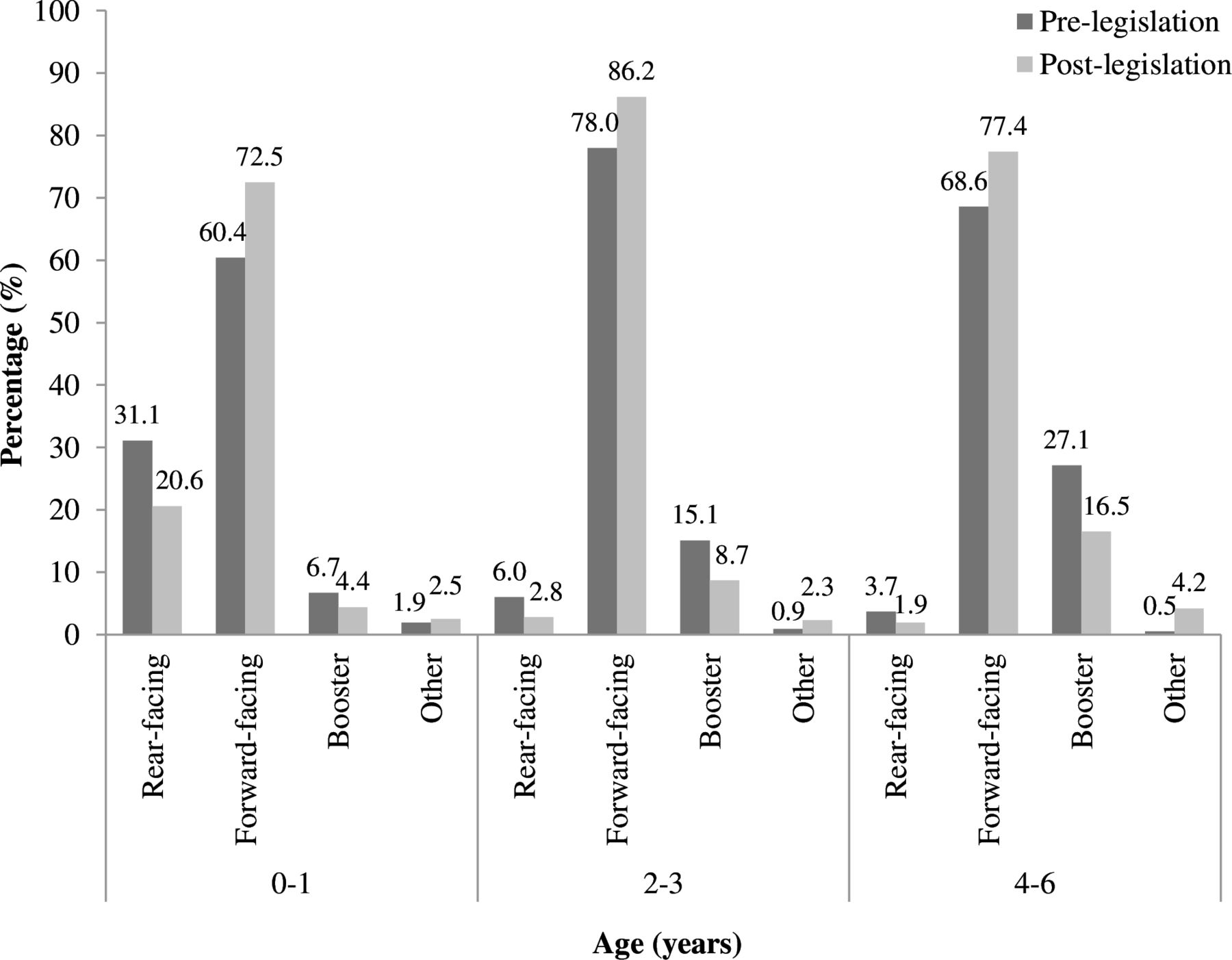
Significant differences were found in the distribution of the types of CRS by age group between the pre-legislation and post-legislation samples. Regardless of age, forward-facing CRS was the main type used for child passengers in both pre-legislation and post-legislation. In addition, the use of booster seats increased significantly with age, with a decreasing trend in rear-facing CRS, particularly in the pre-legislation sample (figure 2).

{kind=link}
{kind=link}
Types of CRS used in the pre-legislation and post-legislation samples in Shenzhen by age group. CRS, child restraint system.
Discussion
To our best knowledge, this is the first study to examine changes in CRS practices among parents in China following the enactment of a local CRS mandatory legislation. The present study demonstrated significant increases in parents owning and using CRS after the implementation of mandatory CRS legislation in Shenzhen in 2015, without locally effective and sustained enforcement. This could be found in children aged below 4 years old and above, respectively. Given the absence of interventions and few public education campaigns on basic knowledge of CRS in the intervening years, the increase in CRS practices here may reflect the positive effect of the local legislation. Nevertheless, the ownership and use of CRS remain quite low in Shenzhen when compared with other high-income countries. For example, among countries that have enacted mandatory CRS laws for decades, the percentage of parents in Belgium owning and using CRS was more than 90%,15 while higher rates of nearly 100% could be observed in Australia.14
As a powerful mechanism for influencing individuals’ behaviours with a significant capacity to improve road safety practices, comprehensive legislation plays an important role in increasing the use of CRS.28 29 This may be because parents are legislatively required to use CRS for their child passengers. Otherwise, they will be fined or receive other penalties.25 However, high rates of legislation compliance are difficult to achieve without education and supportive programmes and enforcement.30 More importantly, without ongoing public education campaigns, the immediate increase of CRS practices accompanying the introduction of the CRS law may not last long.31 These findings highlight the need for greater efforts to improve parents’ CRS possession and use in Shenzhen to protect child passengers from injuries and deaths due to motor vehicle crashes.
It is well documented that CRS offers a high level of protection for child occupants in the event of road traffic crashes. However, the crash protection effectiveness of CRS may be compromised by inappropriate and incorrect use.32 33 Optimal CRS use requires that child passengers be restrained in CRS appropriate for their age and size and used in line with the manufacturer’s instructions,34 but suboptimal CRS practices appear to be a widespread and long-standing problem worldwide. Earlier reports have indicated that the rates of misuse and inappropriate use of CRS were quite high, even in high-income countries where child restraint laws have been in place for a long time.34 35 To gain the full benefit and best levels of protection, the proportion of parents using CRS appropriately and correctly should be closer to 100% and be sustained over time.34 Despite a significant improvement in CRS possession and use in this study, we observed a reduction in child occupants who were restrained appropriately after the enactment of local mandatory legislation. This may be because people need to have CRS fitted properly and appropriate instruction provided as to use especially if families have never used them before. There is an urgent need for further targeted efforts to obtain and sustain a high level of appropriate CRS use.
In contrast, the self-reported correct CRS use rate was extremely high in both pre-legislation and post-legislation samples in the present study. It is important to note that this measure was based on the response to a question asking whether the restraint was used and installed in line with the manufacturer’s instructions. Thus, this trend should be interpreted cautiously since we could not entirely preclude the possibility that parents might overestimate it due to self-confidence or social desirability. A filed inspection study where the quality of restraint use is directly observed is needed to evaluate the actual status of appropriate and correct CRS use in Shenzhen.
Previous studies noted that combining education with restraint subsidies could boost the rate of appropriate CRS use effectively and hands-on fitting programmes and community-based interventions could make a significant difference in correct CRS use.36 37 However, to date in Shenzhen, public education has been limited and neither hands-on campaigns nor loan or rental programmes have been established locally. Thus, effective comprehensive countermeasures are urgently required to improve child occupant safety in Shenzhen.
Notwithstanding the progress signified by the introduction of mandatory CRS legislation in Shenzhen, several shortcomings of the legislation should be noted. The current legislation mandates CRS use for child occupants under the age of 4 years and remains ambiguous on the age-appropriate CRS that parents should choose for their children. From the data collected in the post-legislation period, there appears to be substantial scope to improve appropriate use by better clarification of what constitutes age-appropriate use within the legislation. Furthermore, the best practice recommended by the WHO is that children should be restrained in an approved CRS at least until they are 10 years old or 135 cm in height.3 This means there is also substantial scope to expand the age groups required to use CRS.
As with all studies, there are several limitations to keep in mind. First, the self-reported data is subject to recall and reporting bias. For example, some parents might over-report CRS behaviours they see as favourable and overestimate the optimality of their CRS practices out of social desirability. However, self-reporting is a practical, feasible and cost-effective way to collect data from a large sample. The results demonstrate that even with this potential bias, which would affect both pre-legislation and post-legislation samples, there is substantial room for improvement in CRS practices in Shenzhen. Second, this study was only carried out in Shenzhen, one of the most developed cities with mandatory CRS legislation in China. This may reduce the representativeness and generalisability of our results. Third, families that met the inclusion criteria were invited to participate in our surveys, and no restriction on the number of eligible children per family included in the sample was made and no attempt to account for data clustered by family was made in the analysis. However, the number of children from the same family was very small in the pre-legislation and post-legislation samples (2 and 10, respectively), and so the effect of this is likely minimal.
Conclusions
Despite improvements in CRS possession and use observed following the implementation of legislation, further efforts to update the local mandatory legislation and implement targeted multifaceted interventions including increased and sustained enforcement of laws are highly needed to increase optimal CRS practices for better child passenger safety in Shenzhen. Meanwhile, this study also provides supportive evidence for the introduction of national laws mandating CRS use in China.
Data availability statement
Data are available upon reasonable request. Data of the research are available upon reasonable request from the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Ethical Review Committee of National Center for Chronic and Non-Communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention (201711) and the Human Research Ethics Committee, University of New South Wales (HC230412). Participants gave informed consent to participate in the study before taking part.
References
Footnotes
X @margiepeden, @rebeccaivers
Contributors WC contributed to formal analysis, data curation and writing-original draft. KP contributed to formal analysis and data curation. YJ and LL contributed to investigation and resources. MT, MP and RQI contributed to writing-review and editing and validation. JP contributed to conceptualisation, methodology, supervision and guarantor. JB contributed to writing-review and editing, validation and supervision. All authors participated in the review of the manuscript, read and approved the final manuscript.
Funding This study was funded by the US Center for Disease Control and Prevention (No. 5U19GH000636), Global Road Safety Partnership (No. CHNXX-RD09-1022) and Shenzhen Medical Key Discipline Construction Fund (No. SZXK065). WC is supported by a Scholarship from the George Institute for Global Health funded by the J & K Wonderland Foundation and Tuition Fee Scholarships from University of New South Wales. JB is supported by an Australian National Health & Medical Research Council Investigator Grant (No. 2027133).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.