Article Text

Abstract
Introduction Suicide is a leading cause of death among Native American youth and adolescents in the USA. A myriad of factors have been correlated with risk for suicide ideation (SI)/suicide attempt (SA), including historical trauma; however, accurate measurement of historical trauma has been inconsistent.
Objective To examine the association of family history of a negative mandatory boarding school experience with SI and SAs.
Methods An anonymous online survey was conducted with 288 Native youth aged 15–24 years from the Fort Peck Reservation in Montana. Multinomial regression was applied adjusting for other known risk and protective factors of SI and SAs.
Results Thirty-five percent reported past SAs and 15% reported ideation without prior attempt. Of the 129 (45%) reporting a family history of mandatory boarding school experiences, 28% perceived the experience as positive while 22% as negative. After adjusting for risk and protective factors, both SI and SAs were associated with a family history of negative mandatory boarding school experiences (adjusted OR (AOR)=4.8 and 4.3, respectively) and polydrug use (AOR=3.6 and 2.3). SAs were also associated with post-traumatic stress disorder (AOR=2.6) and depressive symptoms (AOR=3.6).
Conclusion The association between family history of negative mandatory boarding school experiences and SI and SAs implies that culturally responsive interventions are needed to reduce the intergenerational impacts of historical trauma.
- suicide/self?harm
- community research
- cross sectional study
- health disparities
- adolescent
Data availability statement
Data are available upon reasonable request. Study data are available upon reasonable request to the Corresponding Author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Over the past several decades, and through the COVID-19 pandemic, Native American adolescent and young adults have experienced the highest rates of suicide mortality and morbidity.
Suicide ideation (SI) and/or suicide attempts (SAs) among adolescents vary greatly by geography, Indian Health Service area and tribe.
Native American youth are exposed to historical trauma and contemporary trauma, among a host of other risk factors, which place them at greater risk for SI and/or SAs.
WHAT THIS STUDY ADDS
This study assesses the association of family history of negative mandatory boarding school experiences, as a novel way of measuring historical trauma, with SI and SAs after adjusting for other risk factors and cultural protective factors.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Study findings have implications for research and clinical practice—to more efficiently identify and proactively provide support to individuals at higher risk for adverse outcomes, such as SI and/or SAs, due to historical trauma.
Introduction
Suicide has been the second leading cause of death for Native American (NA) youth 15–24 years of age for almost 40 years.1 NAs (American Indian/Alaska Native) have experienced the highest rates of suicide mortality and morbidity in the USA. In 2021, age-adjusted suicide rates were highest among NA persons overall; and this group experienced the highest relative percentage increase during 2018–2021 (from 22.3 to 28.1 per 100 000; a 26% increase).2 Results from the 2021 Youth Risk Behaviour Survey (YRBS) showed 27% of NA students considered attempting suicide in the past year, 22% planned for suicide in the past year and 16% attempted suicide.3 The suicide rate (all ages) in the Billings Indian Health Service (IHS) Area, where this study was conducted, was 27.2 per 100 000 individuals.4
A prominent feature of the epidemiology of suicide among NAs receiving care from the IHS is the variation in suicide mortality rates across tribal settings.4 5 Suicide rates and prevalence vary by 10-fold across the 12 IHS Areas and First Nations (FN) in Canada, underscoring the importance of understanding and addressing local contextual factors.4
Risk and protective factors
Correlates of suicide ideation (SI) and suicide attempts (SAs) among NA populations are post-traumatic stress disorder (PTSD), depression, alcohol and/or drug misuse, history of abuse, stress, perceived discrimination, aggression, exposure to a loved one’s suicide, family history of mental health problems, criminal involvement and low socioeconomic status.6 7 The 2021 YRBS also found NA youth were more likely than other groups to experience forced sexual acts and electronic bullying.3 Additional risk factors unique to NA populations include living on a reservation and personal/family history of attendance in a government-run boarding school.8–11 Factors associated with lower prevalence of SI/SA include connectedness to school and culture, family cohesion, communal mastery, benevolent peer-to-peer relationships, social support, spirituality and emotional well-being.9 10 12
US government termination and assimilation policies, such as mandatory boarding school attendance, have been linked with Historical Trauma (HT) is hypothesised as a contributor to the burden of health disparities among NAs.13 For our context, we are referring only to events which occurred in the USA (1878–1920), whereby the government forcibly removed an estimated 65495 children from their families and placed them in government/parochial-run schools designed to assimilate children through elimination of tribal identity, values, traditions, and language.14 Children were disconnected from family/community and sometimes experienced additional traumas such as malnutrition and abuse.14 15 These experiences were detrimental to the formation of identity, self-esteem, and positive parent–child bonds.15
In North American studies exploring the relationship between elements of HT and suicide, HT has been operationalised by historical loss16; having had a caretaker who attended boarding school17; and personal or family history of boarding school attendance.15 18 Findings have been inconsistent, due in part to operationalisation and sample sizes. For example, a Canadian study explored direct and indirect exposure to effects of boarding school in a random sample of 1125 on-reserve FN adolescents from 23 communities in seven tribal areas. Half the sample had a parent/grandparent attend residential school, but this was not associated with lifetime suicidal behaviours.12 A second study with 2953 on-reserve FN adults found SI and SA were significantly related to having a parent or grandparent who attended residential school, but not personal residential school attendance.18 Further analyses stratified on boarding school attendance showed that SI and SA were not associated with self-reported negative health effects from boarding school nor multigenerational exposure among attendees. However, both SI and SA were associated with multigenerational exposure for non-attendees.18 In the USA, HT and mental health were examined among 447 urban, NA, two-spirit (LGBTQIA+) adults, whereby HT was associated with greater likelihood of generalised anxiety disorder, PTSD and SI, but not SA.17
Study purpose
One explanation for inconsistencies may be that boarding schools varied across regions/tribes and by positive/negative experiences. HT may predispose individuals to disparate outcomes, particularly in the presence of contemporary trauma(s) affecting many NA people.4 19 To the authors’ knowledge, no other study has examined the indirect connection between a family history of negative boarding school experiences with suicide-related behaviours among NAs. Therefore, the purpose of this study was to examine the association of a family history of negative mandatory boarding school experiences (HT) with SI and SA.
Methods
Conceptual framing
Based on prior studies with NAs and guidance from local tribal leaders, we developed a conceptual model to guide our aims and hypotheses (figure 1). We hypothesised that the impact of HT on subsequent suicidal behaviour would be impacted by risk and protective factors and are described below in this fashion.

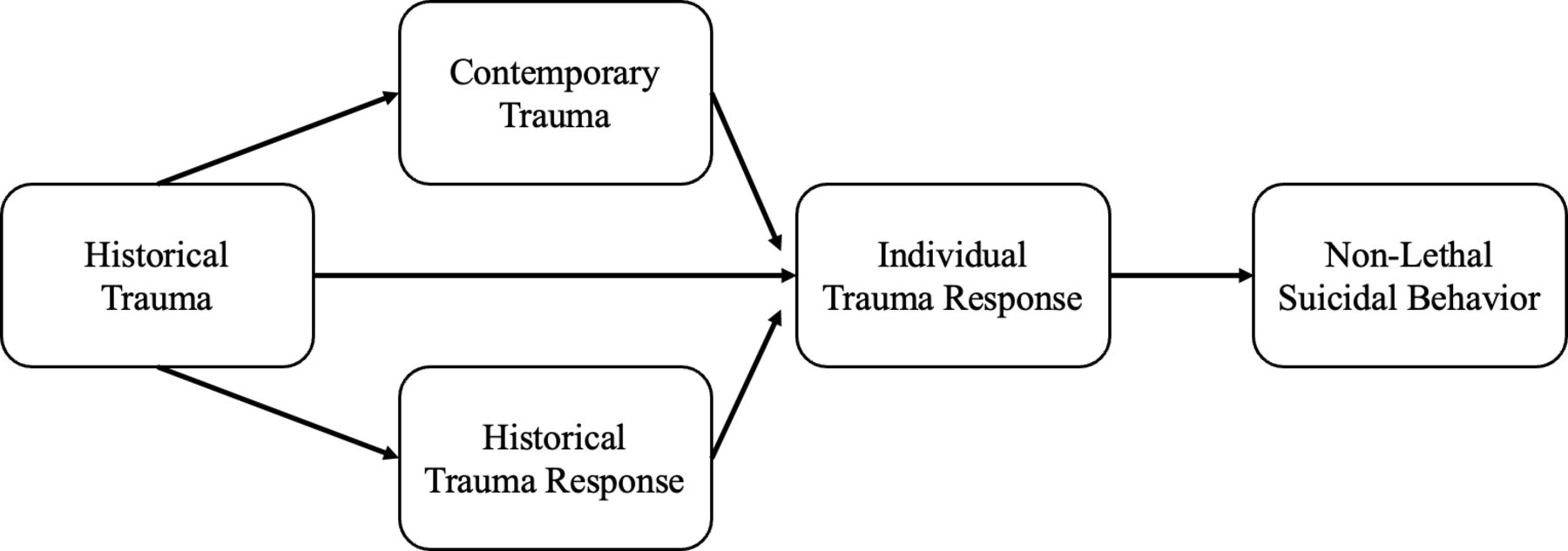{kind=link}
Conceptual model: historical and contemporary factors that influence non-lethal suicidal behaviour among reservation-based NA youth. Note: Historical Trauma (HT) is the collective experience of violence perpetrated on Indigenous Peoples in the process of colonising the Americas that resulted in an unresolved humanitarian crisis for reservation communities, including mandatory boarding school. HT response is the collective mourning of loss of tribal identity and territory, including increased morbidity and mortality. Contemporary trauma is the current occurrences of violent and non-violent trauma experienced by reservation-based NAs, including discrimination. Individual trauma response is the individual response to historical trauma, contemporary trauma and historical loss, including post-traumatic stress disorder. Non-lethal suicidal behaviour includes both suicide ideation and suicide attempt.
Setting and design
The two-million-acre Fort Peck Indian Reservation, located in the Billings IHS Area, is home to the Nakoda (Assiniboine) and Dakota (Sioux) Nations. The reservation lies within a county listed among the poorest and least healthy in the USA.20 Tribal leadership declared a state of emergency in 2010 after 6 suicides and 20 suicide attempts occurred over a 5-month period.
We conducted this analysis using cross-sectional data which were captured as part of a larger study.21 Participants 15–24 years of age completed an anonymous, self-administered questionnaire. An a priori power analysis leveraging the general guidelines of minimum number of events per variable required for model building was conducted; this showed at least n=167 participants were needed.
Public involvement
Local tribal leaders were involved in study design and conduct. A cultural broker was assigned by the Fort Peck Tribal Health Department, who provided guidance and facilitated approval of research-related documents and variable selection. A Tribal Advisory Board (TAB) comprised of local stakeholders and community leaders was also formed.22
Data collection
To be included, participants had to provide written informed consent, and those < 18 years of age required parental/guardian consent/assent. Our safety protocol entailed that all participants live within 1 hour of an IHS facility in case any follow-up for mental/behavioural health was needed. Data were collected in local schools; all questionnaires were completed on paper and uploaded into an electronic, secured database for analysis.
Measures
Primary dependent variables of interest were lifetime SI and SA, which were elucidated by the following questions: ‘Have you ever thought about committing suicide?’ and ‘Have you ever attempted suicide?’ which were modified from another study.23 The primary outcome was a three-level, mutually exclusive variable: (1) non-ideators/non-attempters (reference group); (2) lifetime SI only; and (3) lifetime SA.
Independent variables were derived from measures previously validated in NA communities, apart from the PTSD measure which has been widely used with other subgroups.24 The primary independent variable was HT—operationalised as a family history of negative mandatory boarding school experiences via three items: (1) Were your great or great-great grandparents part of the mandatory boarding school experience? (Y/N); (2) Was this experience talked about in your home? (Y/N); and (3) Did you perceive this experience to be positive, neutral, or negative? We conceptualised HT as a family history of negative mandatory boarding school experiences only, and we differentiated those from positive (i.e., no experiences of abuse) and neutral (i.e., not deemed positive or negative by an individual) with guidance from our TAB members for the purpose of our analysis. Covariates were selected based on available literature and with guidance from our TAB.
Risk factors
Contemporary trauma was operationalised as (1) childhood trauma, (2) exposure to violence, and (3) perceptions of discrimination. Childhood trauma was measured by the Childhood Trauma Questionnaire Short Form (28 items; α=0.92)25 indicating five categories of presence or absence of abuse and neglect: emotional abuse (≥9), physical abuse (≥8), sexual abuse (≥6), emotional neglect (≥10) and physical neglect (≥8). Exposure to violence was measured with a modified version of the 18-item Exposure to Violence scale (α=0.83). Three subscales distinguish types of exposure to violence: witnessing (seven items; α=0.71); being a direct victim (seven items; α=0.70); and learning of violence (four items; α=0.69).26 Additionally, exposure to bullying was assessed by the Y/N question ‘Have you been bullied in the past year?’ and exposure to domestic violence by ‘In your whole life, have you ever seen your mother hit, slapped, punched or beaten up?’ Perceived discrimination was measured using Whitbeck and colleagues’ 10-item perceived discrimination scale (α=0.87).27
Additional risk factors assessed were: (1) PTSD, (2) depression and (3) substance use. We assessed PTSD using the PTSD Screening Scale as a continuous variable.23 Depressive symptoms were assessed using the Beck Depression Inventory (BDI-IA) (21 items; α=0.89); we created a dichotomous variable based on the cut-off score of ≥14 which distinguishes depressed from non-depressed.28 Lifetime-inhalant, methamphetamine, marijuana, alcohol use and prescription drug misuse were assessed (binary variable) by questions adapted from the Centers for Disease Control and Prevention YRBS.29 For context, polydrug use was defined as those with high alcohol use (>100 times), high marijuana use (>100 times) and lifetime use of one of the following: inhalants, methamphetamines or prescription drugs. A binarised approach captured a wider range of individuals who qualified as poly-drug users.
Protective factors
Based on our conceptual model, we hypothesised communal mastery and tribal identity are important considerations for the relationship between HT and SI/SA after adjusting for age, gender, and tribal affiliation. Communal mastery was assessed using the 10-item Communal Mastery Scale (10 items; α=0.85).30 Tribal identity was assessed using a modified version of the 6-item Oetting and Beauvais Orthogonal Cultural Identification Scale (α=0.81) measuring personal and family involvement in Assiniboine and Sioux tribal culture.11
Statistical analysis
We first examined the influence of each proposed risk and protective factor on SI and SA at the bivariate level using multinomial regression. We adjusted p values using Bonferroni correction to account for multiple comparisons; statistical significance was set to p<0.0022. Variables significantly associated with SI and SA were then included in a multivariate analysis, adjusting for covariates of age, sex and tribal affiliation. The final model examined the association of HT on SI and SA, adjusting for age, gender, tribal affiliation and risk and protective factors. All statistical analyses were performed using SPSS, V.19.0.
Results
Complete sample (n=288) demographics are shown in table 1 by SI, SA and No SI/SA. The lifetime prevalence of no SI/SA (reference group), SI only and SA was 50%, 15% and 35%, respectively; overall SI prevalence was 45% (including those with and without SA). We found no demographic differences among the three groups.
Sample characteristics: overall, SI only, SA and no SI/SA
In our assessment of HT, 45% of participants reported a family history of mandatory boarding school attendance, while 15% said they had no history, and 39% were unaware. Of those who reported family history (n=129), 88% indicated the boarding school experiences were discussed at home; further, 38% (n=39) perceived the boarding school experience of their family member as positive, 35% (n=36) as neutral, and 27% (n=28) as negative, respectively.
Five risk factors were statistically significantly associated with SI and 11 with SA in the bivariate model table 2. None of the protective factors were significantly associated with SI or SA after Bonferroni correction. Covariates with a p value <0.002 were retained in the final multivariate model. HT was higher in females (15%) than males (6%) (adjusted OR (AOR)=2.4, p<0.04) and higher in those with greater (16%) versus less (8%) than high school education (AOR=2.3, p<0.04).
Multinomial analysis for SI only (n=44) and SA (n=100) each as compared with no SI/SA
The final model includes constructs significantly associated (p<0.05) with lifetime SI and SA (table 3). Younger age (15–19 years) (AOR=3.6), HT (AOR=4.8) and polydrug use (AOR=3.6) were associated with higher odds of SI. Those with HT (AOR=4.3), polydrug use (AOR=2.3), PTSD symptoms (AOR=2.6), and depression symptoms (AOR=3.6) had higher odds of SA.
Final models for SI only (n=44) and SA (n=100)
Overall, there were minimal amounts of incomplete/missing data. Childhood trauma had the greatest proportion of missing values (13%). The missing data for each variable were determined to be Missing Completely at Random; thus, we limited each analysis to complete cases only.
Discussion
Compared with the National Comorbidity Survey Replication Adolescent Supplement 2001–2002 estimate, we found a considerably higher prevalence of lifetime SI (45% vs 12%) and SA (35% vs 4%).31 Our SA estimate is higher than any recent study using a reservation-based youth sample, but similar to the rate for young Aboriginal injection drug users in Canada.8 10 32 We found no significant sex differences for SI/SA, which is inconsistent with some studies that found females to be at higher risk for SI/SA.10–12 31 Tribe 1 reported a far higher prevalence of HT than Tribe 2 (71 vs 30%), however, we did not find any tribal differences for SI/SA. This may be due to proximity of the two groups residing on the same reservation.
We hypothesised SI/SA may be partially attributable to a family history of negative mandatory boarding school experiences. Attributable risk was 0.97 (CI=0.1385), suggesting negative boarding school experiences account for roughly 10% of SI/SA. However, when we distinguished between positive/neutral and negative mandatory boarding school experience in our operationalisation of HT, we found a significant relationship with lifetime SI and SA when adjusting for other contemporary risk and protective factors. This unique approach could help explain previous inconsistent findings reported on the links between HT and SI/SA. Our findings are consistent with Elias and colleagues’ association between boarding school/multigenerational boarding school experiences and current SI/SA18; but not with Mota and colleagues who found no association.12 Distinguishing between positive/neutral and negative boarding school experiences was critical to understanding how experiences such as this could relate to SI and SA.
Our finding suggests that (1) having a great or great-great grandparent who attended mandatory boarding school over a century ago, and (2) who perceived the experience as negative, was an independent risk factor for SI/SA among this sample. Importantly, 40% of our sample had no knowledge of any boarding school experience, and among the subsample in which this experience was discussed at home, 58% perceived their family members’ experience as positive or neutral. When negative, the boarding school experience operationalisation of HT was more salient to the outcomes than that of HT as historical loss. Negative boarding school experience significantly predicted both SI/SA after controlling for other covariates. Further analysis revealed a greater proportion of those with negative boarding school experiences were also classified as polydrug users. Since polydrug use was strongly associated with SI and SA in bivariate analyses, the relationship between negative boarding school experiences and suicide-related outcomes could have been suppressed by polydrug use. However, we found no evidence that HT, as operationalised in our study, potentiates a more severe response to current traumatic events. None of the proposed HT and contemporary trauma relationships were significant, although limited power could be responsible.
Polydrug use was independently associated with SI/SA in bivariate and multivariate analyses, consistent with other studies.33 At the bivariate level, we found inhalant use and prescription drug misuse increased the odds of SI; while methamphetamine, marijuana, inhalant use and prescription drug misuse increased the odds of SA. Collectively, polydrug use was associated with fivefold increased odds of both SI/SA when compared with non-poly-drug use.
PTSD and depression symptoms were both independently associated with SA, a finding shown in other samples.6 8 14 17 18 Specific forms of trauma exposures were not linked with SA in the final multivariate model. This finding is consistent with results from an urban community sample of young adults and adults with recurrent early-onset depression.34 However, the number of participants in our sample exposed to each trauma was small, limiting the power to detect significant differences relative to sequelae of PTSD and/or depression symptoms. Both PTSD and depression symptoms remained independently associated in the final model for SA, but not SI, similar to findings from other populations experiencing trauma, where PTSD and depression are co-morbid.34
Taken together, our results suggest that HT is a critical variable in understanding current risk factors for reservation-based youth. While our study did not elucidate mechanisms by which HT affects SI/SA, our unique incorporation of the cultural transmission of trauma into our operationalised definition of HT suggests future studies should address this component. Possible mechanisms could involve: (1) intergenerational epigenetic transmission, (2) HT as a marker of poor family functioning, (3) social transmission factors and (4) increased rates of contemporary trauma through intergenerational transmission of violence/trauma. Wakĥàŋyeža (Little Holy One) is one example of an intervention that is prioritising the four mechanisms noted above.35 For example, our team directly used findings from this study to develop cultural content on healing HT given its association with SI and SA. Implemented with parents and their children (3–5 years of age), Wakĥáŋyeža was intentionally designed to foster positive parenting and reduce suicidality. We posit all four of the pathways above should be considered in the development of additional culturally based interventions to reduce intergenerational impacts of HT.
Although we examined two potentially important and conceptually relevant protective factors (communal mastery, tribal identity), neither were significantly associated with SA or SI. As such, results underscore the importance of further research to identify specific protective factors which may interact in the pathway between HT, SI, and SA among NA populations.
Limitations
This study should be contextualised within the scope of its limitations. We used a cross-sectional survey design, which involved self-reported results from those living on one reservation and within 1 hour from an IHS facility, limiting the ability to generalise to other NA communities. In addition, lack of internet access resulted in a low response rate for two of the communities; thereby, our results are subject to selection bias. Finally, there was considerable overlap in the trauma-related variables resulting in multicollinearity in the final model, and we measured lifetime suicidality versus an individual’s momentary status. Future research using structural equation modelling in larger, multi-site samples would better enable identification of mediators/moderators. Additionally, the differences and fluctuation in suicide longitudinally, across geographical areas, and among various subgroups of people (eg, LGBTQIA+/two spirit individuals) calls for inclusion of social and access to care factors such as stigma, economic and geographic/environmental disadvantage in future work.
Nonetheless, our study provides insights on HT and SI/SA among high-risk NA adolescents and young adults and directions for future research addressing this critical issue. Despite ongoing health disparities, there are sources of strength we are only beginning to understand, such as tribal identity, family and community connectedness, and communal mastery.9 12 36
Conclusions
This is one of the first studies to explore the relationship between HT and SI/SA in a high-risk reservation sample. Findings have diverse implications, particularly for those involved in healthcare provision. Practitioners must identify those with potential HT consequences and other risk factors and proactively intervene. Development of upstream interventions targeting resource-limited areas to prevent suicide is imperative to break the complex cycle of multigenerational risk.
Data availability statement
Data are available upon reasonable request. Study data are available upon reasonable request to the Corresponding Author.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Tribal Resolution (#25-1707-2011-02) authorised the study. The Johns Hopkins University Institutional Review Board approved the study (Protocol # NA_00039213), and it was reviewed by a tribal designee from Fort Peck reviewed and approved all research documents. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We gratefully acknowledge the Dakota and Nakoda Nations of the Fort Peck Reservation, including participants and leaders, who made this work possible. In addition, we acknowledge and appreciate Michael R Phillips, MD, MA, MPH for his invaluable expertise and comments during the preparation of this manuscript, as well as Deana Around Him, Miriam Magaña López and Li Yang for their cultural and content expertise.
References
Footnotes
X @DrHollyWilcox
Contributors Guarantor: TB; Indigenous expertise: TB, JI, LWetsit; Public health content expert: LWissow, GW, HW; Suicide content expert: LWissow, HW; Conceptualisation: TB, JCC, GW, HW; Statistical analysis: TB, JI, KN; Manuscript drafting and editing: TB, JCC, JDI, KN, HW; Overall revisions and proofs: JI, KN, HW.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.