Article Text

Abstract
Background Traumatic brain injury (TBI) is an acute injury that is understudied in civilian cohorts, especially among women, as TBI has historically been considered to be largely a condition of athletes and military service people. Both the Centres for Disease Control and Prevention (CDC) and Department of Defense (DOD)/Veterans Affairs (VA) have developed case definitions to identify patients with TBI from medical records; however, their definitions differ. We sought to re-examine these definitions to construct an expansive and more inclusive definition among a cohort of women with TBI.
Methods In this study, we use electronic health records (EHR) from a single healthcare system to study the impact of using different case definitions to identify patients with TBI. Specifically, we identified adult female patients with TBI using the CDC definition, DOD/VA definition and a combined and expanded definition herein called the Penn definition.
Results We identified 4446 adult-female TBI patients meeting the CDC definition, 3619 meeting the DOD/VA definition, and together, 6432 meeting our expanded Penn definition that includes the CDC ad DOD/VA definitions.
Conclusions Using the expanded definition identified almost two times as many patients, enabling investigations to more fully characterise these patients and related outcomes. Our expanded TBI case definition is available to other researchers interested in employing EHRs to investigate TBI.
- Traumatic Brain Injury
- Cohort Study
- Epidemiology
- Standards
Data availability statement
We will make all relevant code and other shareable resources available on our GitHub page: https://github.com/bolandlab.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Traumatic brain injury (TBI) surveillance and research in the USA has focused mainly on youth and young adults from athletic and combat-veteran populations. A gap in knowledge exists for TBI among women across the lifespan, who may be diagnosed in hospital settings outside of these populations.
WHAT THIS STUDY ADDS
We found that prior definitions did not capture all TBI diagnosed in our community hospital setting, and our expansive definition yielded a larger cohort of female patients than would have been obtained if we had used either the Centres for Disease Control and Prevention or the Department of Defense/Veterans Affairs TBI definitions alone.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
By using an inclusive case definition, we were able to identify a larger number of female patients with TBI, representing a distinct, and potentially understudied TBI patient population. Our method and definition is useful and important for other researchers and clinicians using Electronic health records from community settings. By focusing on community settings, where female patients are typically diagnosed, we are also highlighting a population under-explored in TBI research.
Introduction
Traumatic Brain Injury (TBI) is an acute injury, defined as an alteration in brain function as a result of mechanical energy transmitted to the head from external forces.1 TBI is prevalent in the USA, where 1.5–2 million Americans experience a TBI annually, and approximately 80% are treated in the emergency department (ED).2 Described as a ‘silent epidemic’,3 TBI is a pervasive and significant public health concern. Yet, our understanding of its epidemiology is limited, particularly among women in community settings. Although recent collaborative efforts have improved TBI surveillance,3 differences defining and classifying TBI, measuring true TBI incidence, and the availability of quality data remain as challenges.1
Importance of studying diverse populations with TBI obtainable from EHRs
Peer-reviewed TBI literature in the USA has focused mainly on young adults from athletic4 and combat-veteran populations,5 where the majority of participants are men. Similarly, in national studies such as the level-1 trauma centre-based Transforming Research and Clinical Knowledge in Traumatic Brain Injury (TRACK-TBI) study, two-thirds of patient-participants are men.6 Therefore, the resulting TBI literature, which informs the identification, treatment, and management of patients with TBI, is heavily male-focused.7–10 Initiatives to study the epidemiology and clinical trajectories of female athletes and combat-veterans with TBI have emerged.11 12 However, more work is needed, particularly among women in community, hospital and outpatient settings. Electronic health record (EHR) data remain an underutilised resource for better understanding TBI in these settings.
TBI definitions from the CDC and DOD/VA
In the ED setting, the Glasgow Coma Scale (GCS) traditionally aids clinicians in classifying TBI by estimating an individual’s clinical status and injury severity, measured via verbal responses, motor responses and eye movement following a TBI.13 14 The GCS score is calculated on a 15-point scale, where 13–15 is mild TBI (mTBI: approximately 80% of all TBIs fall into this category), 9–12 is moderate TBI (approximately 10% of all TBIs), and ≤8 is severe TBI (also roughly 10% of all TBIs).1 15
Aligning with this classification by GCS, the US Centers for Disease Control and Prevention (CDC) and Department of Defense (DOD)/Veterans Affairs (VA) developed their own surveillance case definitions to classify TBI severity in the EHR using International Classification of Diseases, 9th and 10th revision (ICD-9 and ICD-10) billing codes. The CDC code sets were designed for emergency admissions to estimate the rate of TBI and exclude patients outside the hospital setting, such as primary care, urgent care, and specialty clinics.
Differences between TBI definitions: TBI severity
There have been efforts to classify TBI along a severity continuum, typically as mild, moderate or severe, according to duration of loss of consciousness and/or presence of post-traumatic amnesia.1 However, the value of these measures as indicators of true severity is questionable, since neither are mandatory diagnostic criteria for TBI.1 Still, the DOD/VA’s surveillance case definition outlines codes in terms of TBI severity (mild, moderate, severe, penetrating, not classifiable).16–18 However, the DOD/VA codes have been validated in the military health system, where patients are predominantly men with health insurance, and may not reflect patients in community settings. A re-examination of these definitions towards an inclusive set of diagnostic codes that capture TBI diagnosed in community settings, that is, the locations where women with TBI are typically diagnosed, is warranted. Importantly, the CDC definition of TBI does not include a breakdown by TBI severity, making it impossible to capture when using the CDC’s definition alone. Thus, we harness both CDC and DOD/VA definitions to create our expansive definition, as described in this paper.
Objective
The purpose of this study was to explore how cohorts change by use of different case definitions for TBI. We also sought to develop an inclusive, expansive definition of TBI that may be applicable to adult female patients identified from hospital electronic health records (EHRs). By using both CDC and DOD/VA TBI case definitions, we compare and highlight potential differences among a cohort of female patients from the EHR of a large university hospital system.
Methods
Patient data source
Our source population consisted of 1 060 100 adult female patients with inpatient or outpatient clinic visits to Penn Medicine. We defined adult as age ≥18 years at the time of TBI diagnosis encounter. We also verified age by determining the time between date of birth and TBI diagnosis encounter to ensure this value matched the patient age recorded at the time of TBI diagnosis encounter. These data were obtained from the Penn EHR from four different hospitals within the Penn Medicine system; Hospital of the University of Pennsylvania, Pennsylvania Hospital, Penn Presbyterian Hospital (level-1 trauma centre) and Chester County Hospital along with several ancillary outpatient clinics and centres.19 Penn Medicine follows standard coding practices, whereby clinical providers report full diagnoses from a healthcare encounter, and professional coders assign as many codes as needed to fully explain the healthcare encounter. All patient diagnoses occurred between 2010 and 2017. The Institutional Review Board (IRB) at Penn Medicine approved this study (IRB protocol #851731, #828000), which is a retrospective analysis of existing clinical records. This study is reported per the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. Patients were not directly involved in the conduct of this research.
TBI surveillance case definitions
We identified patients with TBI using International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) and ICD, 10th Revision (ICD-10-CM) billing codes. We extracted patient demographic information from encounter records. We used ICD-9-CM and ICD-10-CM codes from CDC20 and US Department of Defense (DOD),21 Department of Veterans Affairs,16–18 surveillance case definitions to identify patients with TBI. The DOD/VA previously assigned TBI severity classifications (mild, moderate, severe/penetrating, unclassified severity) to each ICD-9-CM and ICD-10-CM diagnosis code,16–18 and we applied this classification to determine TBI severity in our cohort among patients meeting DOD/VA and CDC definitions. Importantly, the CDC does not provide mapped TBI diagnosis codes with TBI severity status. We were only able to map CDC TBI patients to known severity when those patients were also identified using DOD/VA criteria.
The Penn definition included CDC and DOD/VA definitions, and some additional codes. We cross-mapped codes between ICD9 and ICD10, which revealed a few TBI-related codes. In total, we identified 181 codes through this process. Since these codes were new (ie, not included in CDC or DOD/VA TBI definitions), we initially coded these patients’ TBI severity as indeterminate, and made them part of our Penn definition. We were able to cross-map some of these codes with known TBI severity when they mapped to a corresponding ICD9/ICD10 code with a severity related to it. Other TBI codes were identified through previously published manuscripts.17 22 23 Ultimately, we identified 77 codes unique to our definition where it was not possible to characterise TBI severity. Therefore, 77 (42.5%) of the 181 new codes that we added in our definition were indeterminate TBI severity.
Cohort sample selection
We first identified patients who were diagnosed with a TBI-related code, including codes for all healthcare encounter types of initial medical care, subsequent encounter, and sequela. To do this, we applied a decision-tree algorithm of TBI date to extract the most severe TBI diagnosis and used the corresponding earliest date of the most severe TBI diagnosis. We excluded patients with GCS-ICD code diagnoses if they did not have a corresponding injury code, as these likely indicate other aetiologies of coma. This yielded a preliminary cohort of 6856 patients with TBI.
Defining outcome death and survival time
We used two sources to determine patient death due to any cause: death in one of our Penn Medicine facilities and the Social Security Death Index (SSDI).24 Penn Medicine periodically links the SSDI with patient records to determine whether patients are currently living or dead for insurance purposes. Survival time was defined as time from TBI diagnosis encounter to death date. In cases where the patient record indicated a patient had died and death date was available, we used that date (n=175). When death date was missing (and patient status was known as dead or living), and to try to account for any potential lag between patient death and that information being provided to the SSDI, we censored both living and dead patients at a fixed date, which was a minimum of six months after the latest TBI diagnosis date in our cohort, and a maximum of five years. When information on death status was unknown (neither confirmed deceased nor living) and death date was missing, we excluded these cases (n=424) after determining via sensitivity analysis that these patients did not differ in terms of TBI severity and age. This resulted in a final cohort of n=6432 patients for analysis. We then stratified our cohort to determine subcohorts of patients by TBI definition (eg, CDC or DOD/VA).
Statistical analysis
We present descriptive characteristics overall and stratified by case definition: (1) CDC or (2) DOD/VA and (3) Penn definition. To examine whether the addition of these codes in our Penn definition was reliable at identifying TBI, we performed a case validation, whereby a board-certified neurologist (ALCS) manually reviewed the charts from a random sample of 50 indeterminate cases that were new (using the Penn definition only, not CDC or DOD/VA). These cases were reviewed based on standard TBI diagnostic criteria.25 26 Results showed percent agreement among our sample as 72% definite and possible/probable TBI, comparable to other TBI validation studies.27 A full list of all ICD9 and ICD10 codes used to define TBI and TBI severity from the EHR are provided in Appendices available on GitHub (https://github.com/bolandlab/TBI_Definition).
To elucidate potential differences in survival among TBI severity groups and across patients meeting the three TBI case definitions, we conducted survival analysis from time of TBI healthcare encounter to outcome death (in years) by TBI severity (mild, moderate/severe/penetrating, indeterminate severity), with administrative censoring at five years following TBI diagnosis. We grouped moderate, severe and penetrating TBI severities together due to small sample sizes. We used Kaplan-Meier curves with log-rank tests to present overall differences in survival time by TBI severity among the three TBI definition groups (CDC, DOD/VA and Penn-definition). We conducted analyses with R version 4.0.3 using the Survival and survminer packages,28 and created Kaplan-Meier curves with ggsurvplot.29
Results
Penn Medicine cohort sample characteristics
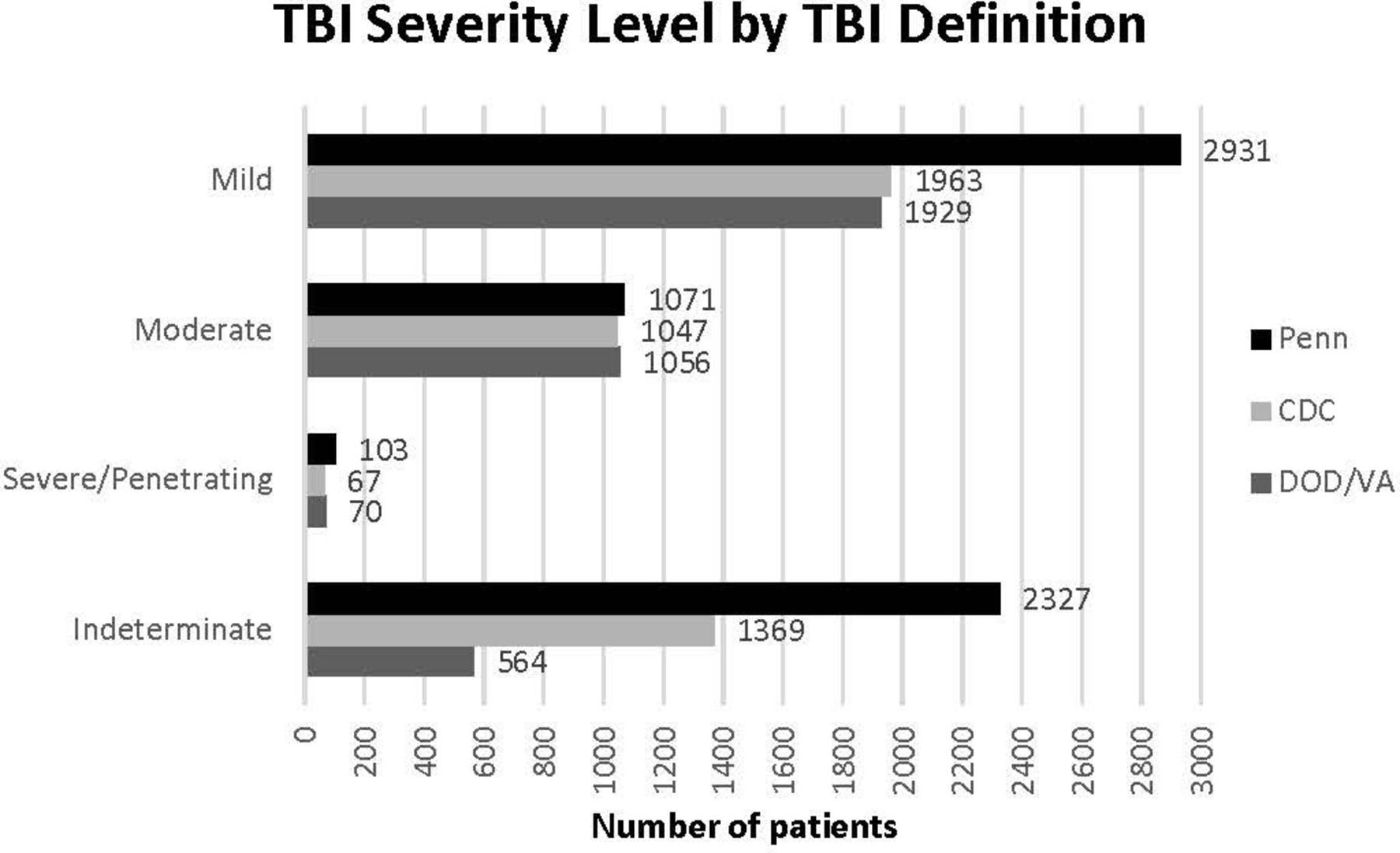
From 1 060 100 adult female patients, we identified 6432 diagnosed with TBI (n=4446 CDC, n=3619 DOD/VA) at Penn Medicine between 2010 and 2017 and and observed their survival over five years. Among them, TBI severity was most commonly mild (n=2931, 45.6%) and ‘indeterminate’ (n=2327, 36.2%). Median age at time of TBI diagnosis encounter was 47 years (25th–75th percentiles: 29–63) and patients were most commonly white (n=4126, 64.0%). Injury mechanism was typically missing in coded data related to the TBI (78.0%), but when present, the most common mechanism was fall (13.0% of all TBIs) followed by collision/crash (2.9% of all TBIs). Around 3% of patients with TBI died within five years (2.7%, n=175). Patient demographic characteristics across TBI case definitions (CDC, DOD/VA, Penn) are presented in table 1.
Overall patient cohort demographics by TBI definition
Differences between TBI definitions in terms of cohort
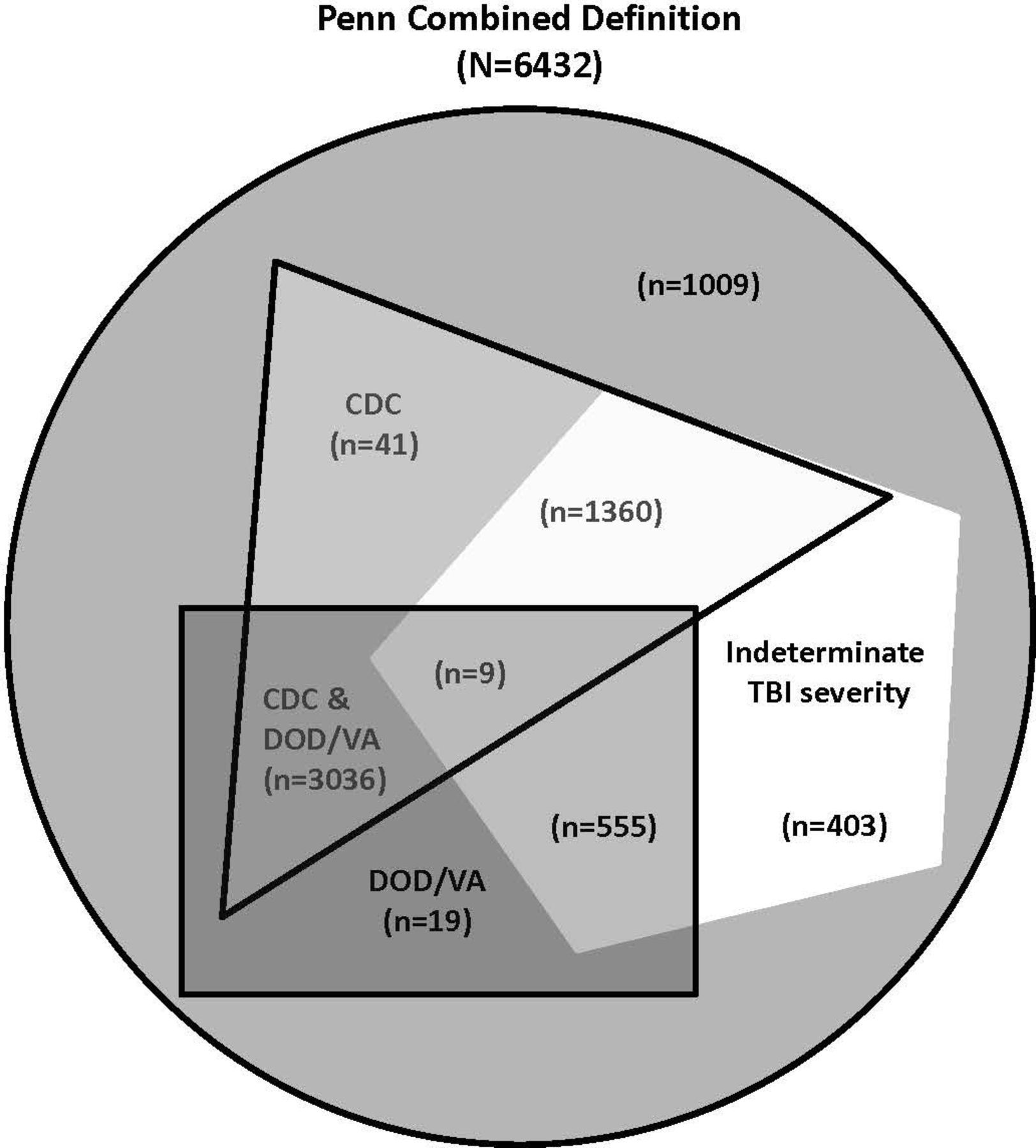
We found some overlap between CDC and DOD/VA definitions (figure 1), including 3045 patients who would be identified as having TBI by both definitions. These 3045 patients were 68.5% of those identified using the CDC definition, and 84.1% of those identified using the DOD/VA definition. Patient age was similarly distributed across definitions (figure 2). Patient TBI severity using the different definitions is depicted in figure 3.

Venn diagram depicting TBI definitions (N=6432). We also include the ‘indeterminate’ TBI severity here to show that the CDC, DOD/VA and our combined Penn definition all include patients that cannot be classified in terms of TBI severity. This diagram is an illustration; please note that shapes in this diagram are not all proportional, for example some shapes are shown to be similar in size when the n is rather different. CDC, Centres for Disease Control and Prevention; DOD, Department of Defense; TBI, traumatic brain injury; VA, Veterans Affairs.

Distribution of age by TBI definition. (A) Penn definition cohort, (B) CDC definition cohort, (C) DOD/VA definition cohort (N=6432). All cohorts are derived from an underlying population of Penn Medicine females. CDC, Centres for Disease Control and Prevention; DOD, Department of Defense; TBI, traumatic brain injury; VA, Veterans Affairs.

Distribution of TBI severity by TBI definition (N=6432). Each cohort is represented: Penn definition cohort, CDC definition cohort, DOD/VA definition cohort. All cohorts are derived from an underlying population of Penn Medicine females. CDC, Centres for Disease Control and Prevention; DOD, Department of Defense; TBI, traumatic brain injury; VA, Veterans Affairs.
Differences in survival among TBI definition group
Overall, there were significant differences in the time from TBI diagnosis encounter to death within five years between TBI severity levels (mild, moderate/severe/penetrating and indeterminate severity) across the three TBI definition groups (CDC, DOD/VA and Penn). The probability of survival at five years was similar across definition groups. Kaplan-Meier curves depicting time from TBI to five-year survival among the three TBI definition groups (panels A, B and C) are presented in figure 4. Note, each panel contains an embedded, scaled version of the figure to assist with readability.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier curves depicting time from TBI diagnosis encounter to death by TBI severity across the TBI case definition groups (A, B, C), N=6432. The shaded bands around each line represent the 95% CIs. At-risk tables for each definition are displayed below each cohort’s Kaplan-Meier curve. Each panel (A, B, C) contains an embedded, scaled version of the figure to assist with readability. CDC, Centres for Disease Control and Prevention; DOD, Department of Defense; TBI, traumatic brain injury; VA, Veterans Affairs.
Discussion
The purpose of this study was to compare existing TBI definitions from the CDC and DOD/VA, which revealed gaps and led to developing an inclusive set of diagnostic codes for identifying TBI in community settings. Our cohort of adult female patients would typically be diagnosed with TBI in community hospital settings, which required an expansive definition of diagnosis codes to capture TBI appropriately. We used the CDC and DOD/VA TBI case definitions, and literature to develop our definition,17 22 23 and highlight potential differences among a female cohort from the EHR at Penn Medicine. This expansive definition yielded a larger cohort than would have been obtained if we used either the CDC or DOD/VA TBI definitions alone. We are not aware of prior studies that have used the CDC and DOD/VA TBI case definitions together, which is a novel contribution.
Differences between cohorts obtained by TBI definitions
We found similarities among patients meeting TBI definitions (CDC, DOD/VA, Penn) in terms of age at TBI diagnosis, race, ethnicity, TBI severity, injury mechanism, visit type (inpatient/outpatient) and provider department. Our findings align with some descriptive studies, demonstrating a bimodal distribution in TBI incidence by age; whereby, TBI incidence is highest during younger and older adulthood.30 31 Our finding that all-cause mortality was associated with TBI severity, regardless of TBI definition, builds on several prior findings of decreased survival associated with TBI among patients with inpatient and outpatient health records data,32 33 and this should be explored further.
Patients of indeterminate TBI severity: not included in DOD/VA or CDC definitions
Our Penn TBI definition (N=6432 patients) yielded a large number of patients with indeterminate TBI severity (n=2327, 36.2%). Some examples include postconcussion syndrome, post-traumatic headache, post-traumatic hydrocephalus, post-traumatic seizures, occipital flow blowout, broken mandible. While in general neurology practice, another corresponding TBI code would typically accompany these injury codes, we found some patients without these TBI codes. One possible explanation is that trauma and emergency medicine clinicians, who are focused on treating the immediate injury, may code these injuries without their corresponding TBI codes. Thus, TBI patients of ‘indeterminate’ severity may actually be patients initially coded by non-neurologist/neurosurgeon specialists.22 34 This is further evidenced by our finding that diagnoses in our cohort were primarily given by either general practitioners or non-neurologist specialists. This has important implications for future TBI research using cohorts from the EHR to consider provider department in the assignment of TBI diagnosis.
Potential for inadequate controls in TBI research studies using EHR data
We identified a group of female patients with ‘indeterminate’ TBI severity, suggesting that existing case definitions may be at risk of missing or misclassifying some patients with TBI. If this is the case, studies utilising these EHR data may not be capturing all patients with TBI. Or if patients with TBI are not coded as such in the EHR, labelled as ‘healthy’, and used as clinical research controls, this has downstream effects including threats of differential misclassification and Berkson’s bias. Future work should consider these findings when designing studies utilising EHR data.
Focus on female TBI patients using existing TBI definitions: CDC and DOD/VA
Existing TBI studies (and case definitions they inform) have focused on specialised athletic or military populations, where patient cohorts are often men, young, otherwise healthy individuals (with the exception of older, veteran populations). Prior studies have also been limited to examining sex as an effect modifier.8 33 The size of our all-female cohort permits us to investigate characteristics within this population.
Limitations and future work
There are some limitations of our work that also spur future research directions. We used two established TBI case definitions from the CDC and DOD/VA, and reviewed additional ICD codes to create a more inclusive definition of TBI based on literature and on the premise that individuals with significant structural or tissue damage (ie, facial fracture/trauma) may be triaged with diagnosis and treatment focusing on the observable injury, and a TBI may be missed. Future work, including clinical validation of patients meeting neither CDC nor DOD/VA TBI definitions, would aid in further testing hypotheses related to these definitions and applications broadly to patients with TBI in community and hospital settings. These steps may also strengthen the clinical utility of our expanded Penn definition. There are some inherent limitations to using ICD codes. Prior literature suggests that ICD code-based TBI definitions are susceptible to misclassification, particularly for mild TBI, with validation studies reporting 55%–72% sensitivity and 80%–85% specificity, depending on the ICD-code definition used.5 27 In this study, we used standard ICD codes as used by the CDC and DOD/VA to identify patients with TBI. Therefore, we did not re-evaluate these code sets but employed them on our cohort. We note the differences in cohort sizes obtained by the different methods. Our cohort includes patients from hospitals, clinics and centres within one large health system in Philadelphia, PA, and results may only be generalisable within the greater Philadelphia area. Much of our sample received a TBI diagnosis from a provider outside of neurology/neurosurgery, primarily general practitioners and other specialists. We consider this an important finding that speaks to diversity in our sample and highlights a subset of patients who may go understudied in TBI EHR research. Our retrospective study limited us to information collected in each patient’s EHR. Finally, we originally hoped to examine injury mechanism, but as noted, this was not included in roughly 70% of our sample. Still, our finding that falls was a common injury mechanism reflects the range of ages in our sample, and is consistent with prior literature.30
Conclusions
In this study, we compared two common methods for identifying patients with TBI, the CDC and DOD/VA case definitions. We developed an inclusive case definition for TBI that combines and expands these definitions and applied it in a female cohort from the EHR at Penn Medicine. In doing so, we identified a larger number of patients with TBI. Others interested in studying TBI using EHRs should consider using this definition (available on GitHub). Also, by focusing on female patients, we highlight an often understudied group in the TBI literature. Our work fills this gap.
Data availability statement
We will make all relevant code and other shareable resources available on our GitHub page: https://github.com/bolandlab.
Ethics statements
Patient consent for publication
References
Footnotes
X @berndalonzo
Presented at Work that motivated the current study has been presented previously at the Society for the Advancement of Violence and Injury Research (SAVIR), and the American Medical Informatics Association (AMIA) annual meetings.
Contributors B.A.D. and M.R.B. conceived of the study design. B.A.D., R.B.M., and M.R.B. developed the methodology with input from S.P.C. and D.J.W. A.L.C.S. conducted the manual chart review and with A.C.B., provided clinical insights pertinent to the study, and interpretation of results. B.A.D. and M.R.B. drafted the manuscript. All authors reviewed, edited, and approved the final manuscript. B.A.D. and M.R.B. accept full responsibility for the work and conduct of the study, had access to the data, and controlled the decision to publish.
Funding The research reported in this manuscript is supported, in part, by the Penn Injury Science Center, which is an Injury Control Research Center funded by the Centers for Disease Control and Prevention, with a pilot grant funding to Dr. MRB (R49CE003083) that covered efforts by Dr. SPC. The research was also supported by the Institutional Clinical and Translational Science Award (CTSA) with Dr. MRB as a co-Investigator (UL1-TR-001878), with Dr. Garret Fitzgerald as PI. Dr. ACB was supported in part by the National Institute of Health–National Institute of Neurological Disorders and Stroke Brain Injury Training Grant (T32 NS 043126). Dr. ALCS is supported in part by NIH grant K23NS123340. Some funding also provided by the University of Pennsylvania via start-up funding to Dr. MRB.
Competing interests ALCS is an Associate Editor at Neurology. DJW provides consulting services on the topic of concussion/TBI epidemiology to the NCAA.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer-reviewed.